
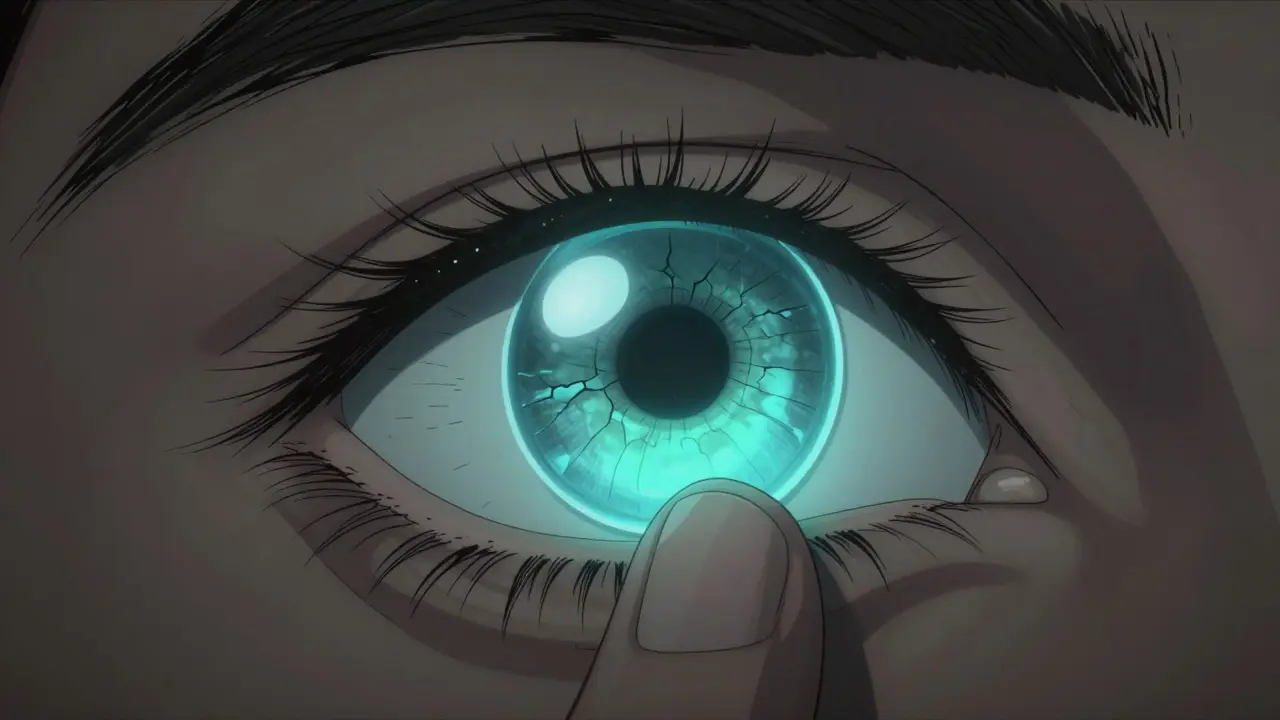
When your cornea starts to thin and bulge outward like a cone, your vision doesn’t just get blurry-it becomes distorted, shaky, and unpredictable. Glasses won’t fix it. Soft contacts won’t stay in place. That’s the reality for people with keratoconus, a progressive eye condition that affects about 1 in 2,000 people worldwide. It usually shows up in the teens or early 20s, and while it doesn’t cause pain, it can steal your ability to see clearly without intervention. The good news? For most people, rigid contact lenses aren’t just an option-they’re the most reliable way to get vision back.
What Actually Happens in Keratoconus?
Your cornea is the clear, dome-shaped surface that covers the front of your eye. It does more than just look pretty-it’s responsible for focusing most of the light that enters your eye. In keratoconus, the collagen fibers that hold the cornea in shape start to weaken. Enzymes break them down faster than the body can repair them. Over time, the center of the cornea thins, stretches, and bulges into a cone shape. This isn’t just a surface change-it alters how light bends as it enters your eye, creating multiple focal points instead of one sharp image. This doesn’t happen overnight. It usually progresses slowly over 5 to 10 years, then stabilizes by the time most people reach their 40s. It often affects both eyes, but rarely equally. One eye might be mildly affected while the other is severely distorted. That’s why people with keratoconus often notice one eye seeing worse than the other, or why they might struggle with glare, halos around lights, or double vision in one eye.Why Regular Glasses and Soft Contacts Don’t Work
Glasses correct vision by bending light evenly across a smooth surface. But when your cornea is irregular, no single lens prescription can fix the multiple distortions it creates. Soft contact lenses, which conform to the shape of your eye, simply follow the cone’s irregular curve. They don’t mask it-they amplify it. That’s why many people with keratoconus report that even their strongest glasses still leave them seeing double or blurry, especially at night. That’s where rigid lenses come in. Unlike soft lenses, rigid gas permeable (RGP) lenses keep their shape. When placed on the eye, they float on a thin layer of tears, creating a new, smooth optical surface over the irregular cornea. Think of it like putting a clear, hard plastic sheet over a crumpled piece of paper-the paper is still wrinkled underneath, but the surface you’re looking through is flat and clear.The Three Types of Rigid Lenses Used for Keratoconus
Not all rigid lenses are the same. There are three main types used today, each suited to different stages of the disease:- RGP lenses (9-10mm diameter): These are the most common starting point. Made from oxygen-permeable materials with Dk values between 50 and 150, they allow enough oxygen to reach the cornea during wear. They’re small, sit directly on the cornea, and offer sharp vision. But they can feel uncomfortable at first, especially if the cornea is already sensitive.
- Hybrid lenses: These combine a rigid center (for clarity) with a soft outer skirt (for comfort). They’re a good middle ground for people who find RGPs too harsh but aren’t ready for larger lenses.
- Scleral lenses (15-22mm diameter): These are the largest and most advanced option. Instead of sitting on the cornea, they vault over it entirely and rest on the white part of the eye (the sclera). A reservoir of saline solution fills the space between the lens and the cornea, acting like a cushion. This not only improves vision but also protects the cornea, reduces dryness, and makes them ideal for advanced cases or those with corneal scarring.
Studies show that scleral lenses have an 85% success rate in stage III-IV keratoconus, compared to 65% for traditional RGPs. For people who’ve tried everything else and still can’t see clearly, scleral lenses often make the difference between functioning normally and being visually disabled.
How Rigid Lenses Compare to Other Treatments
There are other ways to manage keratoconus-but none offer the same combination of vision correction and non-invasiveness as rigid lenses.- Corneal cross-linking (CXL): This is the only treatment proven to stop keratoconus from getting worse. It uses UV light and riboflavin (vitamin B2) to strengthen the collagen fibers in the cornea. It’s highly effective-90-95% of patients see progression halt after treatment. But CXL doesn’t fix your vision. You still need lenses afterward.
- INTACS: These are tiny plastic rings inserted into the cornea to flatten its shape. They help some people, but 35-40% still need rigid lenses after the procedure.
- Corneal transplant: This is the last resort. About 10-20% of people with keratoconus eventually need a transplant, either replacing the full cornea (PK) or just the front layers (DALK). Recovery takes over a year. There’s a 5-10% risk of rejection. And even after a transplant, many patients still need rigid lenses to get the clearest vision.
Rigid lenses don’t cure keratoconus. But they don’t need to. Their job is to restore vision, and they do it better than anything else for most people.
What to Expect When You Start Wearing Rigid Lenses
Adapting to rigid lenses isn’t like switching to a new pair of glasses. It takes work. Most people start with 2-4 hours of wear per day, then add an hour every couple of days. Full-time wear-8-12 hours a day-usually takes 2 to 4 weeks. About 85% of patients eventually get there. In the first week, common complaints include:- Foreign body sensation (45% of new wearers)
- Feeling the lens move or being aware of it (38%)
- Difficulty inserting or removing the lens (32%)
These aren’t signs of failure-they’re signs of adjustment. Most people stop noticing the lenses after a few weeks. The vision improvement, though, is immediate and dramatic. Many go from seeing 20/400 without correction to 20/200 or better within days of fitting. Long-term users often reach 20/25 vision, which is considered normal.
Common Problems and How to Fix Them
Even after adaptation, issues can pop up:- Lens fogging (25% of users): Caused by protein buildup or oil from eyelids. Switching to a preservative-free cleaning solution helps.
- Lens decentration (15%): The lens shifts off-center. This usually means the fit needs adjusting-your eye care provider may need to tweak the curve or diameter.
- Solution sensitivity (10%): Some people react to preservatives in lens solutions. Switching to preservative-free rewetting drops or saline can solve it.
Regular follow-ups are key. A good fitting process involves 3-5 visits over 4-6 weeks. Corneal topography scans are used to map your eye’s shape and design the perfect lens. Manufacturers like BostonSight (PROSE) and Contex offer custom digital designs now, where lenses are made based on your exact corneal scan-something approved by the FDA in early 2023.
Who Needs Scleral Lenses Over RGP?
You don’t need to jump straight to scleral lenses. Most eye doctors start with RGPs because they’re cheaper, easier to fit, and work well for mild to moderate cases. But if you have:- Advanced corneal thinning
- Scarring on the cornea
- Severe dry eye
- Pain or discomfort with RGPs
then scleral lenses are likely your best bet. They’re more expensive and require more expertise to fit, but they’re also more forgiving. The fluid reservoir keeps the eye moist, reduces irritation, and provides stability even if the cornea is very irregular.
Long-Term Outlook
Keratoconus doesn’t go away, but it doesn’t have to control your life. Rigid lenses have been the standard of care for decades-and they’re getting better. New materials now allow oxygen permeability (Dk) values over 200, meaning longer, safer wear. Digital manufacturing means lenses fit more precisely than ever. Most eye specialists now recommend combining rigid lenses with corneal cross-linking. The lenses give you vision. The cross-linking stops it from getting worse. Together, they offer the best long-term outcome. About 70% of people diagnosed with keratoconus end up using rigid lenses long-term. Only 10-20% ever need surgery. That means for the vast majority, the answer isn’t a scalpel-it’s a small, clear lens that sits on the eye and changes everything.If you’ve been told your vision can’t be corrected, or if your glasses feel like they’re not doing enough, ask your eye doctor about rigid lenses. They’re not glamorous. They take effort. But for thousands of people every year, they’re the thing that lets them drive, read, work, and see their children’s faces clearly again.
Can keratoconus be cured with rigid lenses?
No, rigid lenses don’t cure keratoconus. They correct the vision problems caused by the irregular cornea but don’t stop the underlying thinning. To halt progression, corneal cross-linking (CXL) is required. Rigid lenses are a visual rehabilitation tool, not a cure.
Are scleral lenses better than RGP lenses for keratoconus?
It depends on the stage of the disease. For early to moderate keratoconus, RGP lenses often work well and are easier to adapt to. For advanced cases with scarring, dry eye, or extreme irregularity, scleral lenses are more effective-offering better comfort, stability, and visual clarity. Success rates for scleral lenses in advanced cases are about 85%, compared to 65% for RGPs.
How long does it take to get used to rigid contact lenses?
Most people need 2 to 4 weeks to adapt. Start with 2-4 hours per day and increase by 1-2 hours every few days. Discomfort, lens awareness, and insertion issues are normal at first. By the end of the fourth week, 85% of patients can wear them full-time without trouble.
Do rigid lenses stop keratoconus from getting worse?
No. Rigid lenses improve vision but don’t affect disease progression. Only corneal cross-linking (CXL) has been proven to stop the cornea from thinning further. Many patients use both: CXL to halt progression and rigid lenses to restore vision.
Can you wear rigid lenses every day?
Yes, most people wear them daily for 8-12 hours. Modern RGP and scleral lenses are designed for extended wear with high oxygen permeability. However, they must be cleaned daily and replaced every 1-2 years. Never sleep in them unless specifically prescribed by your eye care provider.
What’s the success rate of rigid lenses for keratoconus?
About 70% of people with keratoconus achieve long-term success with rigid lenses. This means they can wear them comfortably every day and maintain good vision without needing surgery. Success is highest when lenses are fitted by specialists using corneal topography and when patients follow cleaning and wear guidelines closely.
Are rigid lenses expensive?
RGP lenses cost $100-$300 per pair and last 1-2 years. Scleral lenses are more expensive, ranging from $800 to $2,000 per pair due to custom fitting and advanced materials. Insurance often covers part of the cost if prescribed for a medical condition like keratoconus. Some providers offer payment plans.
Can you drive with keratoconus and rigid lenses?
Yes, most people with rigid lenses can drive safely. Once vision is corrected to 20/40 or better-which most achieve with proper lens fitting-driving is not restricted. Many patients report improved night vision and reduced glare after switching from glasses to rigid lenses.

Janette Martens
December 28, 2025 AT 14:58PS: I still typo everything but my vision? 20/20. LOL.
Marie-Pierre Gonzalez
December 30, 2025 AT 02:00Thank you for this exceptionally well-researched and compassionate overview. As a long-term scleral lens user, I can attest that the saline reservoir is nothing short of miraculous for dry eyes.
While adaptation requires patience, the transformation in quality of life is profound. I now read bedtime stories to my daughter without straining-something I feared I’d never do again.
With profound gratitude for medical innovation and dedicated eye care professionals,
Marie-Pierre
Louis Paré
December 31, 2025 AT 00:27Meanwhile, a $2000 plastic disc that sits on your eye like a tiny satellite is the real MVP?
And the fact that this only works because the cornea is too messed up for soft lenses to even cling to? That’s not a fix. That’s a workaround with a price tag.
Also, why is no one talking about how these lenses are made in China? Just saying.
sonam gupta
December 31, 2025 AT 18:33Julius Hader
January 1, 2026 AT 08:04Don’t give up. Your eyes deserve this fight.
oluwarotimi w alaka
January 2, 2026 AT 20:23Debra Cagwin
January 4, 2026 AT 10:52I’ve coached dozens of people through this. The first week is the hardest. The second month? You’ll forget you’re wearing them.
Find a specialist who uses corneal topography. Ask for payment plans. Reach out to support groups. You deserve to see clearly. Keep going.
Bradly Draper
January 6, 2026 AT 05:26